A recent review article published in the New England Journal of Medicine, looked at currently available and emerging pharmacological antidotes to reverse anticoagulation in patients with major bleeding or those requiring urgent surgery.
There is an increasing use of anticoagulants worldwide, especially with the introduction of DOACs, and although they have a lower bleeding risk, overall more patients are using them, which has led to more patients presenting with severe bleeding.
THE STUDY
Rocca B and Cate H. Antidotes for Anticoagulation Reversal. NEJM 394;22 June 11, 2026. pp.. 2235-2254.
Choosing the appropriate reversal agent depends on:
- The anticoagulant being taken
- The pharmacology of the antidote
- The urgency of bleeding or surgery
- Patient-specific factors (renal function, thrombotic risk)
- Availability and cost of reversal agents
WHAT THEY DID
Thiw was an evidence review of:
- Randomised controlled trials
- Observational studies
- Systematic reviews and meta-analyses
- Pharmacokinetic and pharmacodynamic studies
- Current regulatory approvals and international guidance
Reversal strategies included:
- Unfractionated heparin
- Low molecular weight heparin
- Fondaparinux
- Vitamin K antagonists (warfarin)
- Dabigatran
- Factor Xa inhibitors (apixaban, rivaroxaban, edoxaban)
- Emerging reversal agents such as ciraparantag and VMX-C001
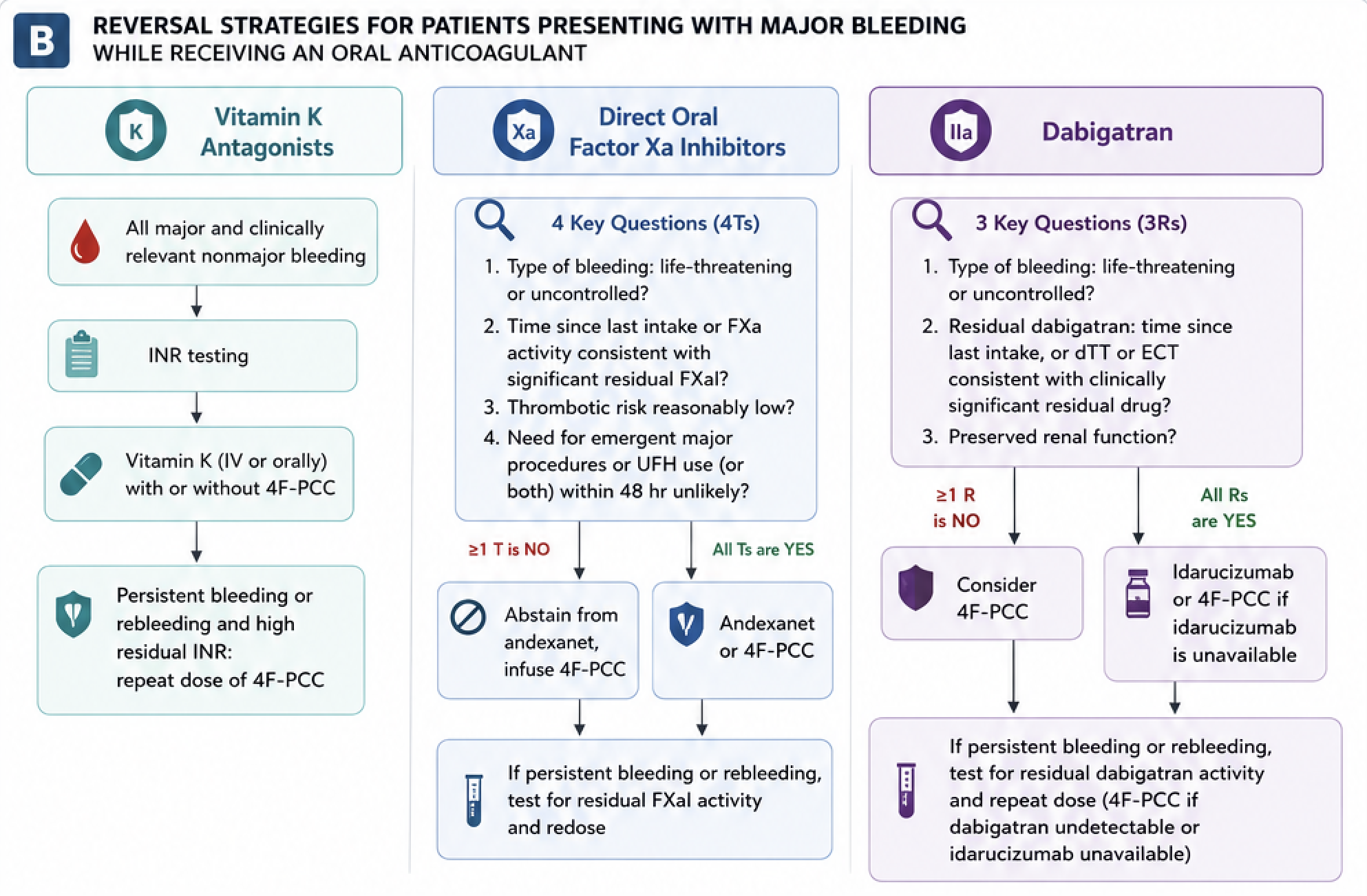
The review also provides practical algorithms, summary tables, and illustrations explaining where each antidote acts within the coagulation cascade.
WHAT THEY FOUND
1. Protamine
- Remains the only specific antidote for unfractionated heparin.
- Only partially reverses low molecular weight heparin.
- Does not reverse fondaparinux.
- Optimal dosing and laboratory monitoring remain uncertain.
2. Vitamin K antagonists (Warfarin)
- Four-factor prothrombin complex concentrate (4F-PCC) plus intravenous vitamin K is the preferred reversal strategy.
- Faster INR correction and improved haemostasis compared with fresh frozen plasma.
- Fixed-dose PCC strategies require further study.
3. Dabigatran
- Idarucizumab provides rapid, almost complete reversal.
- Highly effective for major bleeding and emergency surgery.
- Some patients experience delayed rebound of dabigatran, particularly with renal impairment, occasionally requiring repeat treatment.
4. Factor Xa inhibitors
- Andexanet alfa rapidly reverses apixaban and rivaroxaban.
- Improves haemostatic efficacy compared with usual care.
- However:
- thrombotic complications are consistently higher,
- mortality benefit has not been clearly demonstrated,
- laboratory monitoring is difficult,
- treatment is expensive,
- and the drug has important regulatory restrictions.
- Because of safety concerns, andexanet was withdrawn from the US market in late 2025, although it retains conditional approval in Europe.
5. Four-factor PCC
- Frequently used off-label for Xa inhibitor-associated bleeding.
- Remains an acceptable alternative where andexanet is unavailable or unsuitable.
- Direct comparative evidence between PCC and specific antidotes remains limited.
Limitations
The review identifies several important limitations in the current evidence base:
- Few adequately powered RCTs.
- Many studies are observational or single-arm without comparator groups.
- Small sample sizes.
- Results related to laboratory markers rather than meaningful patient-centred outcomes.
- Non-standard definitions of haemostatic efficacy across studies.
- Short follow-up periods, making long-term thrombotic risk uncertain.
- Limited evidence for emergency surgery.
- Lack of validated laboratory assays to monitor reversal of factor Xa inhibitors after andexanet.
- Very limited head-to-head comparisons between PCC and specific antidotes.
RECOMMENDATIONS
- Use the correct antidote for the specific anticoagulant whenever possible.
- Reserve andexanet for carefully selected patients with life-threatening bleeding after balancing thrombotic risk.
- Continue using 4F-PCC for warfarin reversal and when specific antidotes are unavailable or inappropriate.
- Individualise treatment according to:
- bleeding severity,
- residual anticoagulant activity,
- renal function,
- thrombotic risk,
- need for urgent surgery.
- Prevent bleeding through optimisation of anticoagulant prescribing, regular review of dosing, management of hypertension, renal disease and drug interactions.
- Develop better laboratory assays, safer antidotes and more robust clinical trials with patient-centred outcomes.
SUMMARY
This is a comprehensive review of anticoagulant reversal. It confirms that:
- Warfarin: 4F-PCC plus vitamin K remains the gold standard.
- Dabigatran: Idarucizumab is highly effective and remains the preferred specific antidote.
- Factor Xa inhibitors: Andexanet provides better laboratory reversal and improved haemostasis but at the cost of increased thrombotic risk, uncertain mortality benefit, high cost and regulatory concerns. 4F-PCC remains the preferred antidote.
The major gap in the field is the lack of high-quality comparative trials evaluating clinically important outcomes rather than surrogate laboratory markers.