The new Clinical Practice Guidelines by the AHA on the Evaluation and Management of Acute Pulmonary Embolism have been published.
Here is a synopsis of those guidelines.
The Paper
Creager MA et al. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2026;153:e00–e00.
INTRODUCTION
The diagnosis of PE is difficult, with less than 10% of the patients evaluated for PE being diagnosed with the condition. The accepted failure rate of diagnostic tests is about 2%. Although the most common symptoms are pleuritic chest pain and dyspnoea, most symptoms are non-specific.
Clinical decision rules such as the Wells Score and the Revised Geneva Score can assist in determining a clinical pre-test probability and the D-dimer can help in further risk stratifying patients.
PE accounts for up to 11% of pregnancy related deaths. We find that a low number of pregnant patients having a CTPA (4.1%), have a positive scan. The D-dimer and the YEARS algorithm lowers the rate of imaging.
NEW CLASSIFICATION OF PE
There is a new classification of PE. The previous low risk, submassive and massive PE, have been replaced by five new categories. This new classification describes severity and prognosis. It appears complex at first. However if we remember that Categories A and B are patients at lower risk of adverse outcomes, Category C are symptomatic patients with increased risk of adverse outcomes depending on cardiac biomarkers and echocardiography and Cateries D and E are the sickest patients at risk of cardiopulmonary failure and arrest.
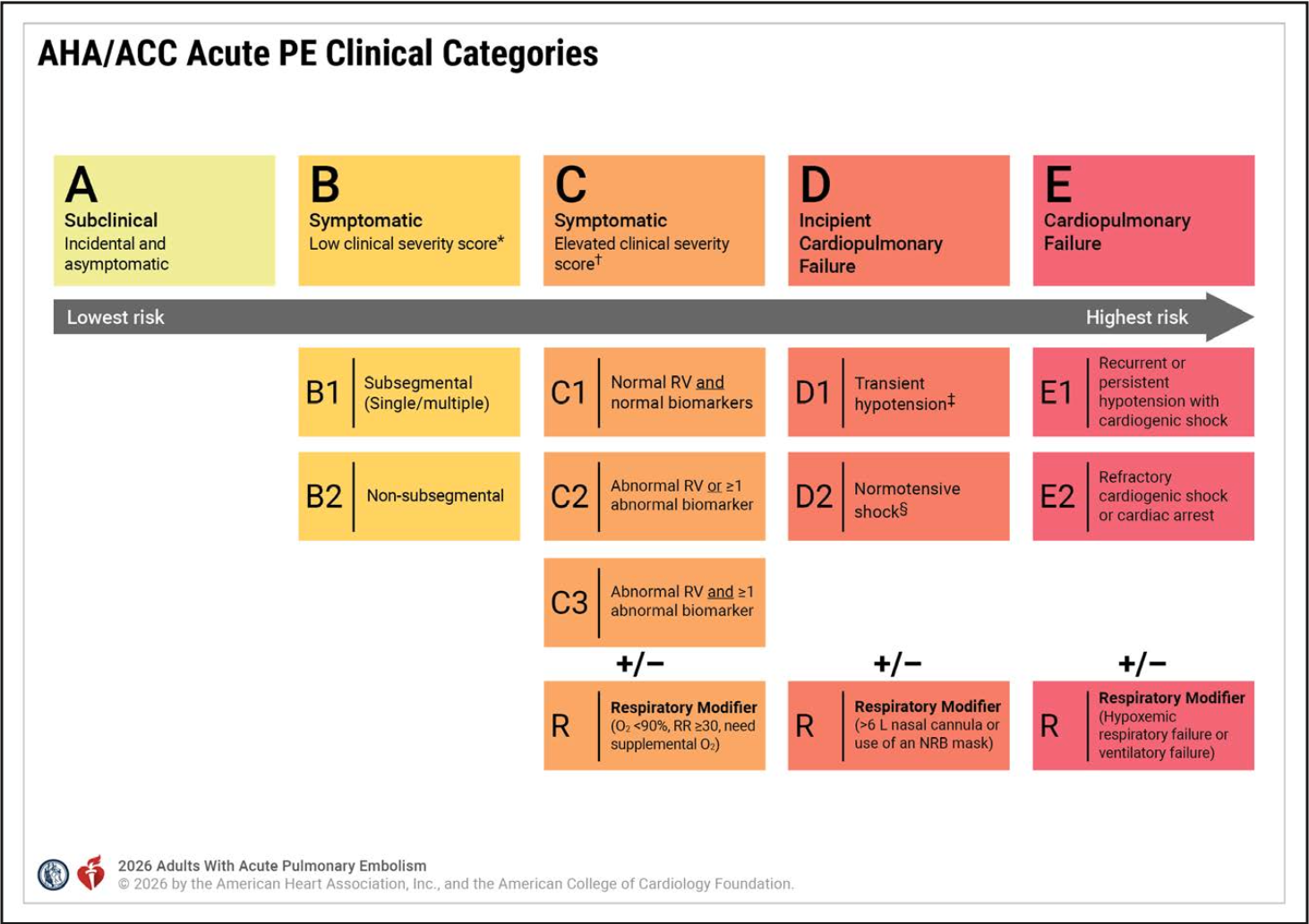
Category A
The least severe category. Patients are asymptomatic and PE is incidentally diagnosed.
Category B
These are patients who have an acute PE and are symptomatic but at low risk of adverse outcomes based on severity indices.
- Category B1
- Patients with single or multiple subsegmental PEs
- Category B2
- Patients with segmental and more proximal PEs.
Category C
Patients with symptomatic disease and an increased risk of adverse outcomes using a validated severity index (eg, PESI >85, sPESI ≥1, Hestia ≥1).
- Category C1
- Normal RV and normal biomarkers(cardiac troponin I/T and brain-type natriuretic peptide)
- Category C2/C3
- Abnormal RV size or function on echocardiogram or CT. The respiratory modifier, R, is applied when hypoxemia or tachypnea is present or there is a need for supplemental oxygen.
Category D
Patients with pre-cardiopulmonary failure states, such as normotensive shock or the developing need for ventilatory support.
- Category D1
- Patients with transient or recurrent hypotension, that is short-lived or responds to volume expansion and is not accompanied by signs of reduced perfusion or end-organ dysfunction.
- Category D2
- This is normotensive shock
- It requires measurement of a marker of decreased perfusion or end-organ dysfunction , such as lactate.
- The respiratory modifier, R, would be applied if the patient required either >6 L nasal cannula or use of a nonrebreather mask.
Category E
This is the most severe category.
- Category E1
- Recurrent or persistent hypotension with cardigenic shock
- Category E2
- This is refractory cardiogenic shock (SCAI D-E) or cardiac arrest without restoration of spontaneous circulation after 30 minutes of resuscitation. The respiratory modifier is defined by the need for non-invasive or invasive positive pressure ventilation.
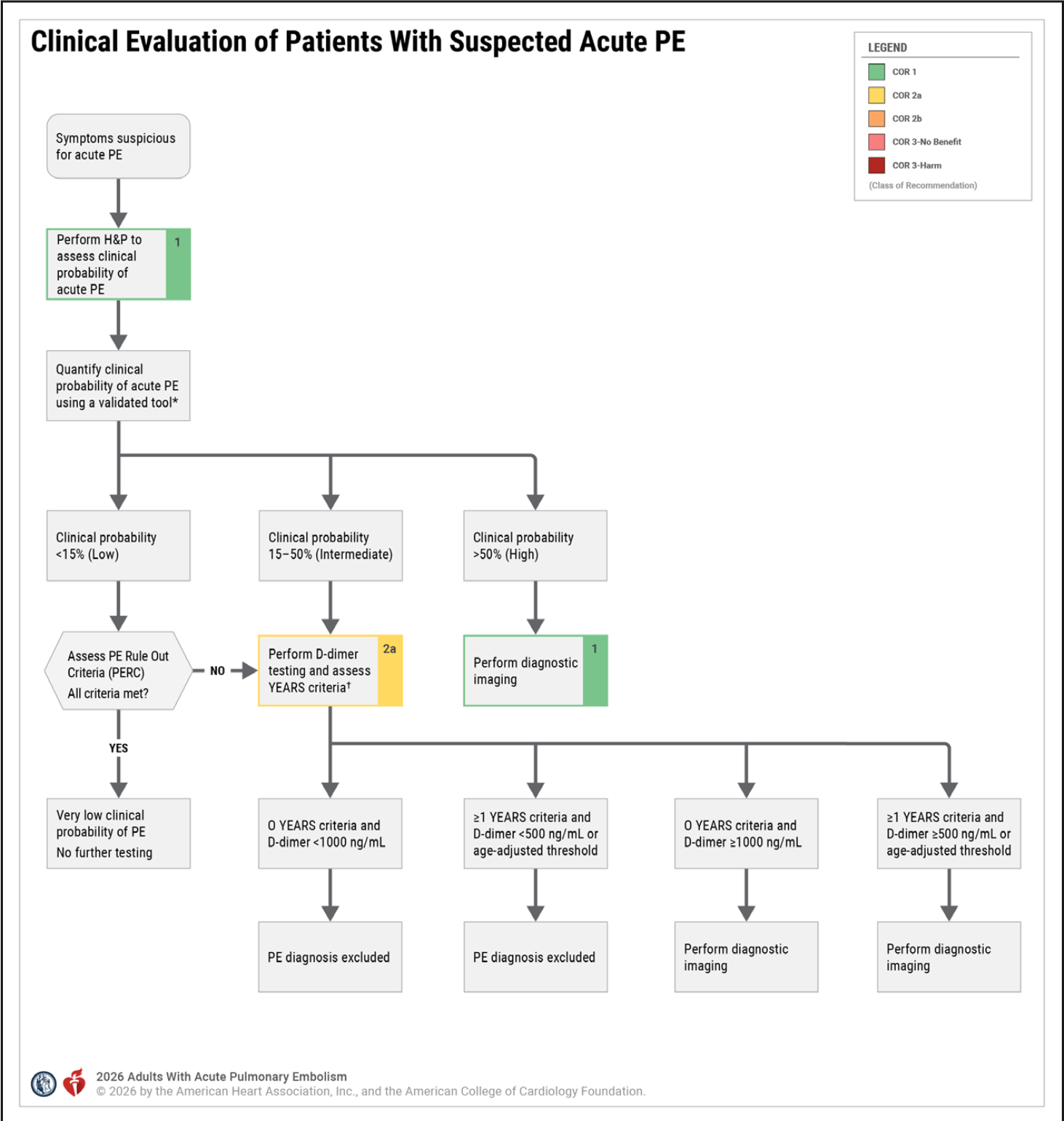
EVALUATION OF THE PATIENT WHERE THERE IS A SUSPICION OF PE
The guidelines recommend the use of clinical probability followed by either the PERC rule of the D-dimer, used with the YEARS criteria, to rule out PE or alternatively to perform imaging. Suspicion of a PE based on the history and examination, requires determination of a pre-rest probability. Validated rules such as the Wells Score and the Revised Geneva Score, as well as our own clinical gestalt, can be used to risk stratify patients.
Gestalt is something we use every day in our clinical practice, however it does depend on our experience. The Wells Score also includes gestalt, in that we need to decide if ‘PE is the most likely diagnosis’. The Revised Geneva Score, is what I personally recommend, as it contains no gestalt, but is based on history and clinical examination findings.
Having said this, if the Clinical suspicion is high for a PE, regardless of what the Clinical Scores show, that patient should be investigated for a PE. Any patient with a high clinical probability needs imaging.
RISK FACTORS FOR PE
- Recent Surgery
- Hospitalisation for medical treatment
- Immobility
- Pregnancy
- Oestrogens
- Trauma
- Cancer
- Inflammatory Disorders
- Inherited and Acquired Thrombophilia
CLINICAL RISK SCORES
WELLS SCORE
- Clinical Signs and Symptoms of a DVT (3 points)
- PE as the #1 diagnosis or as likely (3 points)
- Heart Rate > 100 (1.5 points)
- Immobilisation of > 3 days or surgery in the previous 4 weeks (1.5 points)
- Previously objectively diagnosed PE or DVT (1.5 points)
- Haemoptysis (1 point)
- Malignancy with treatment within 6 months or palliative (1 point)
< 4 : PE is unlikely and a D-dimer can be used to determine if imaging is necessary.
> 4 : PE is likely and imaging is required.
REVISED GENEVA SCORE
- Age >65 (1 Point)
- Previous DVT or PE (3 points)
- Surgery (anaesthesia) or lower limb fracture in the past month (2 points)
- Active Malignant Condition (2 points)
- Solid or hematologic malignant condition, currently active or considered cured <1 year
- Unilateral Lower limb pain (3 points)
- Haemoptysis (2 points)
- Heart Rate
- <75 bpm (0 points)
- 75-94 (3 points)
- >95 (5 points)
- Pain on lower limb palpation and Unilateral Oedema. (4 points)
< 3 points: there is a low probability of a PE ie., <10% chance. Perform a D-dimer
4-10 points: Intermediate risk (20-30% probability): Image these patients
>11 points: there is a > 60% probability of a PE: Image these patients.
OTHER CRITERIA USED IN DECISION MAKING DURING EVALUATION
PERC RULE
In low clinical probability patients(<15%), the PERC RULE can be used to rule out PE.
To be able to rule out PE with the PERC rule, all the following must be negative.
- Age > 50
- HR > 100 (At any time)
- O2 sat on room air < 95%
- Unilateral Leg Swelling
- Haemoptysis
- Recent Surgery or Trauma
- Surgery or Trauma < 4 weeks ago, requiring general anaesthesia
- Prior PE or DVT
- Hormone use
- Oral contraceptives, hormone replacement or oestrogenic hormones use in male or female patients.
If the patient can be ruled out with the PERC rule, nothing further is needed. If they cannot, then they move to the intermediate clinical probability group, where a D-dimer and YEARS criteria are use.
YEARS CRITERIA
YEARS Criteria are used with a D-dimer
There are 3 YEARS Criteria are:
- Clinical Signs of a DVT
- Haemoptysis
- PE is the most likely diagnosis (gestalt again enters the equation)
No YEARS criteria present:
If the D-dimer is:
- < 1000 ng/mL: PE is excluded
- >1000 ng/mL the patient requires imaging
>1 YEARS Criteria present
If the D-dimer is:
- <500ng/mL or age adjusted is normal then PE is excluded.
- >500ng/mL or age adjusted is high then imaging is required.
INVESTIGATIONS
- Cardiac Biomarkers such as Troponin and BNP identify patients at risk of short term complications and mortality.
- Lactate can give clues into subclinical end-organ hypoperfusion. It is important to perform in normotensive patients.
- Echocardiography and chest CT are recommended for patients with acute symptomatic PE and an elevated severity score.
RISK SCORES
Risk Scores identify patients with a low risk of short term adverse outcomes.
Hestia, PESI and sPESI can all identify low risk patients who can be treated as outpatients.
Hestia Criteria
All criteria must be negative for the patient to be considered for outpatient management.
The Criteria are:
- Is the patient hemodynamically unstable?
- Is thrombolysis or embolectomy necessary?
- Does the patient have active bleeding or a high risk of bleeding?
- Does the patient require >24 hours of oxygen to maintain oxygen saturation >90%?
- Is pulmonary embolism diagnosed during anticoagulant treatment?
- Does the patient have severe pain requiring intravenous pain medication for >24 h?
- Are there medical/social reasons for hospitalization >24 hours (eg, infection, cancer, lack of support system)?
- Does the patient have a creatinine clearance of <30 mL/min?
- Does the patient have severe liver impairment?
- Is the patient pregnant?
- Does the patient have a documented history of heparin-induced thrombocytopenia?
PESI Criteria
There are 5 classes of severity:
Class I (lowest risk): ≤65pts
Class II: 66-85 pts
Class III: 86-105 pts
Class IV: 106-125 pts
Class V: (highest risk)≥126 pts
The Criteria are:
- Age Calculate score by adding age (in years) and points by risk factor
- Male (10 pts)
- History of cancer (30 pts)
- History of heart failure (10 pts)
- Chronic lung disease, (10 pts)
- Heart rate ≥110 bpm (20 pts)
- Systolic blood pressure <100 mm Hg (30 pts)
- Respiratory rate ≥30 bpm (20 pts)
- Temperature <36°C (20 pts)
- Altered mental status (60 pts)
- Oxygen saturation <90% (20 pts)
sPESI Criteria
Add 1 pt for each of the risk factors
0 points: Low risk of 30-day mortality
≥1 point: High risk of 30-day mortality
The Criteria are:
- Age >80 yrs
- History of cancer
- Chronic cardiopulmonary disease
- Systolic blood pressure <100 mm Hg
- Heart rate ≥110 bpm
- Arterial oxygen saturation <90%
ACUTE PE TREATMENT OPTIONS
Anticoagulation
Anticoagulation of patients is the mainstay of treatment. More invasive techniques can also be added depending on the classification severity.
Categories A and B: Patients who are asymptomatic, or symptomatic with a low clinical severity score, can be treated with DOAC and are suitable for outpatient management.
DOACs and VKAs are contraindicated in pregnancy as they pose risks to the fetus as they cross the placenta.
DOACs are contraindicated in patients who are breastfeeding, as they may be excreted into breast milk.
Categories C to E: All other categories of patients can have LMWH, have cardiac biomarkers and a lactate measured. They will also need to have RV size and function assessed.
Categories D and E: Patients will require systemic thrombolysis and those in E1 may require surgical embolectomy
Haemodynamic Support
Noradrenaline(NA) is considered the vasopressor of choice. At doses < 15mcg/min it has no effect on PVR. So it increases SVR/PVR ratio. At levels above 15mcg/min, NA begins to increase PVR. A second vasopressor like Vasopressin can be added at this point. In patients with low cardiac output and hypotension dobutamine may be added to NA.
Selective pulmonary vascular dilatation can also be used (mostly ICU).
Cardiovascular Support
Mechanical circulatory support may be used for patients with cardiogenic shock, with evidence of RV dysfunction.
Systemic Thrombolysis
It may improve pulmonary obstruction, with a reduction in RV dilatation on seen on echocardiography.
Agents used are:
- Streptokinase
- Urokinase
- Alteplase (rt-PA) 100mg in 2 hours.
- Tenecteplase
Catheter Directed Thrombolysis
This usually used in Category E1 patients ie., those with cardiopulmonary failure.
Mechanical Thrombectomy
There are no trials comparing the effectiveness of mechanical thrombectomy to systemic thrombolysis.
Surgical Embolectomy
There are no prospective randomised trials comparing surgical embolectomy with other treatment approaches.
POST ACUTE PE MANAGEMENT
Outpatient follow-up is needed to assess symptom improvement, anticoagulation adherence and appropriateness and to look at the potential future course of the condition.
Most patients with uncomplicated PE can be seen by their local doctor.
Patients should be referred to speciality clinics if:
- The have complex anticoagulation management requirements\
- VTE history or recurrent PE
- Unresolved symptoms
- Pregnancy-related PE
- Complicated clinical presentation
- Expert second opinion is needed
PATIENT ACTIVITY AND TRAVEL
Early mobilisation following anticoagulation reduces venous stasis.
Patients will usually be on a 3-6 month course of anticoagulants. Those who have ceased their anticoagulation and are travelling, may benefit from a one time dose of anticoagulant (LMWH or a DOAC) if travelling for long distances ie >4hr flight.