Ohle R, et al. Development of a Clinical Risk Score to Risk Stratify for a Serious Cause of Vertigo in Patients Presenting to the Emergency Department. https://doi.org/10.1016/j.annemergmed.2024.06.003. Article in Press.
The aim of this study was “to prospectively assess the clinical characteristics of patients presenting with vertigo to the ED and to derive a clinical risk score to identify high- and low-risk patients for a serious cause of their vertigo.”
What They Did
This was a prospective multicenter cohort study, conducted in three Canadian Emergency Departments. It included adult patients ( > 17 yo) presenting with acute vertigo, dizziness, or imbalance.
What They Found
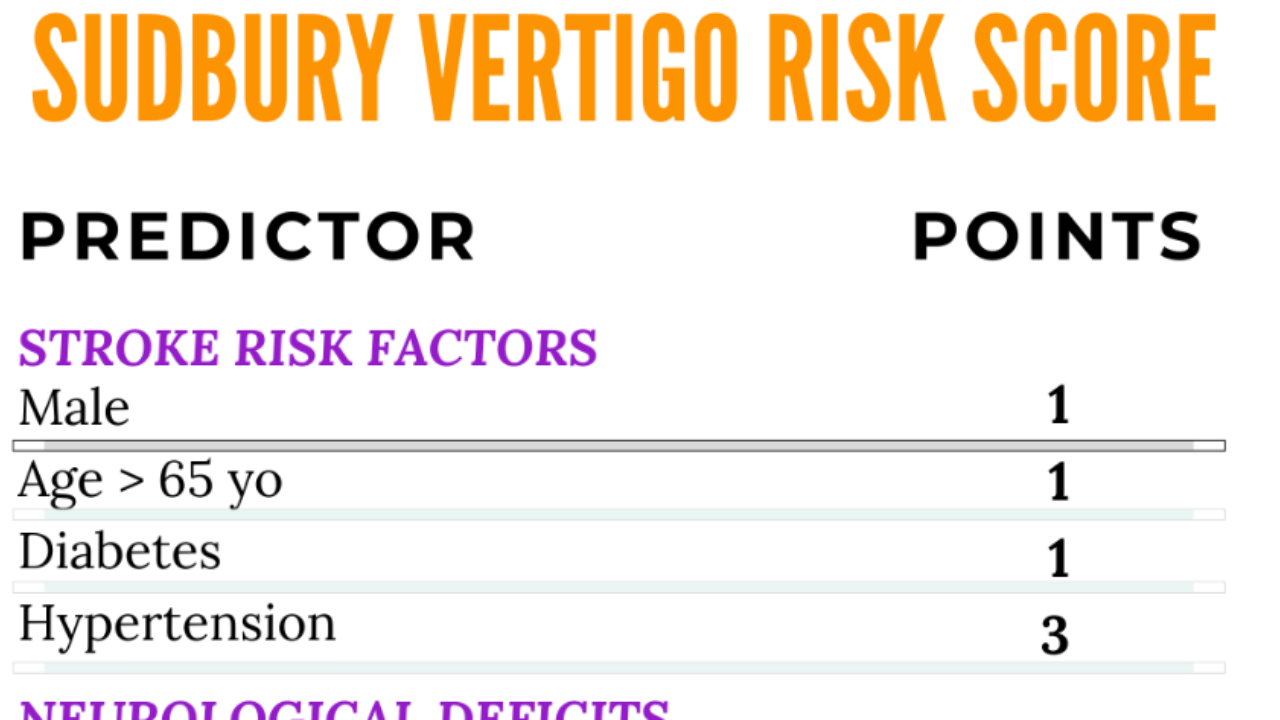
They concluded with a predictive score as below:
Probability of a serious cause (stroke, TIA, vertebral artery dissection, or brain tumor)
- 0% for a score of <5,
- 2.1% for a score of 5 to 8, and
- 41% for a score >8
In this new study they applied the score to a new group of patients presenting with dizziness.
The Validation Study
Tissot van Patot E et al. Validation of the Sudbury Vertigo Risk Score to risk stratify for a serious cause of vertigo. Acad Emerg Med. 2025;00:1–11.
What They Did
This was a retrospective multicenter cohort study in the Emergency Departments of 3 Canadian tertiary care teaching hospitals.
N = 4559 patients
Primary Outome Measure: A diagnosis of stroke, TIA, vertebral artery dissection, or brain tumor diagnosed in the ED or within 30 days of the initial assessment.
What They Found
104 (2.3%) patients had a 'serious' diagnosis:
- 91 (2.0%) had a stroke
- 6 (0.1%) had a TIA,
- 5 (0.1%) had a brain tumor, and
- 2 (0.04%) had a vertebral artery dissection
1678 (36.8%) CT scans, 349 (7.7%) CT angiographies, and 253 (5.5%) magnetic resonance imaging scans were performed.
They found that:
- A score of <5 had a 0% risk of serious outcome: sensitivity of 100% (95% confidence intervals [CI]96.5%–100%) and a specificity of 69.2% (95% CI 67.8%–70.51%).
- 45% of all imaging was performed in this low risk group.
- A Score of 5-8 had a 0.9% risk of serious outcome.
- A Score > 8 had a 16.7% risk of serious outcome.
- A threshold of >7, had a sensitivity for a positive finding on CT of 100% (95% CI 94%–100%) and a specificity of 84.2% (95% CI 83.1%–85.2%).
My Take on This
This is a retrospective analysis, in Canada and at the same sites used for the derivation study. There is no external validation. The outcome assessment is incomplete, potentially affecting results, ie., increasing sensitivity.
The diagnosis of BPPV, carries a -5 value in this score and was determined by a positive Dix-Hallpike or supine roll manoeuvre. We are unsure of how this was performed and if the noted results were accurate.
Let's look at what this may look like in a normal patient.
A 72 yo presents with dizziness for 2 days. It is worse on lateral head movement. There is no real nystagmus and the rest of the examination is normal. The patient has a previous history of ACS, hypertension, diabetes and a right Fem-Pop bypass and is a smoker. He has had a cardiac stent 10 years ago and a kidney transplant 2 years ago. Dix Hallpike is negative but the supine test is positive. The patient is also dizzy when he sits up from a lying position and has a postural BP drop of 15 mm Hg. The neurological examination is normal.
According to the score he receives
- Male: 1 point
- >65 yo:1 point
- Hypertension: 3 points
- Diabetes: 1 point
- BPPV Diagnosis as the supine roll test is positive: -5
He Sudbury score is 1; ie zero percent risk of a serious diagnosis.
Would you be concerned? This is someone that is a vasculopath with significant risk factors for stroke. The one item that gives him a low risk score is the diagnosis of BPPV, which is made on a supine head roll test.
I like what the score is trying to do. At this point I would use it as an exit score ie., if I decide to send the patient home, I'll just check that I haven't missed anything important. I'll wait for the external validation before I apply it.