A 78 yo patients presents with tachycardia and hypotension. There has been a recent episode of dysuria and the diagnosis of urosepsis is made. Antibiotics are given as you give a 500mL fluid challenge with normal saline and the blood pressure responds….briefly. You continue the fluid challenge, each time there is a transient increase in blood pressure.
You decide to commence Noradrenaline and you escalate the dose. The patient’s blood pressure is not responding as needed, so you add Vasopressin. The patient is responding, but you are reaching high levels of vasopressors.
We know that high doses of vasopressors can have adverse effects, including peripheral ischaemia, arrhythmias, and myocardial depression and increased mortality……. enter methylene blue. Can this make a difference?
Sepsis is associated with abnormal nitric oxide metabolism, increased vasodilatation and increased vascular permeability. Methylene blue inhibits nitric oxide synthase and can restore vasoregulation.
In this review we look at a 2023 study on early adjunctive use of methylene blue in septic shock(1). Prior to this there were two randomised controlled trials (2, 3) in 2001 and 2002. In 2004 a large randomised control trial (4) using a non-selective nitric oxide synthase inhibitor was terminated early due to an increase in mortality.
In the study reviewed below, methylene blue was used, which is a specific inhibitor of the inducible isoform of nitric oxide synthase and has been shown to restore vasoregulation where there has been nitric oxide upregulation
What they did
This study asked the question: Can early addition of methylene blue reduce the total time of administration of vasopressors in patients with septic shock?
It was a double blinded, parallel, randomised controlled trial, in one centre.
Patients included were:
- > 17 years old
- Had sepsis requiring noradrenaline (within 24 hours of commencement) to maintain a MAP of >65 mm Hg and had a lactate of > 2mmol/L after fluid resuscitation.
Patients were assigned to two groups:
- Methylene blue group
- Received 100mg of methylene blue in 500ml 0.9% sodium chloride solution over 6 hours per day for three days.
- Control group
- Received 500ml of 0.9% sodium chloride solution
Both groups received vasopressin at 0.03 IU/min when the dose of noradrenaline had reached 0.25 mcg/kg/min
All patients received hydrocortisone (200mg/day) by continuous infusion.
Primary outcome: Discontinuation of all vasopressors for at least 48 consecutive hours.
Secondary Outcomes: Vasopressor free days at 28 days / all-cause mortality at 28 days / serum lactate levels / days on a mechanical ventilator / length of stay in ICU and hospital / change in creatinine, bilirubin, aspartate and alanine aminotransferase / PaO2 to FiO2 ratio and ejection fraction following intervention.
N = 91
What they found
Primary Outcome
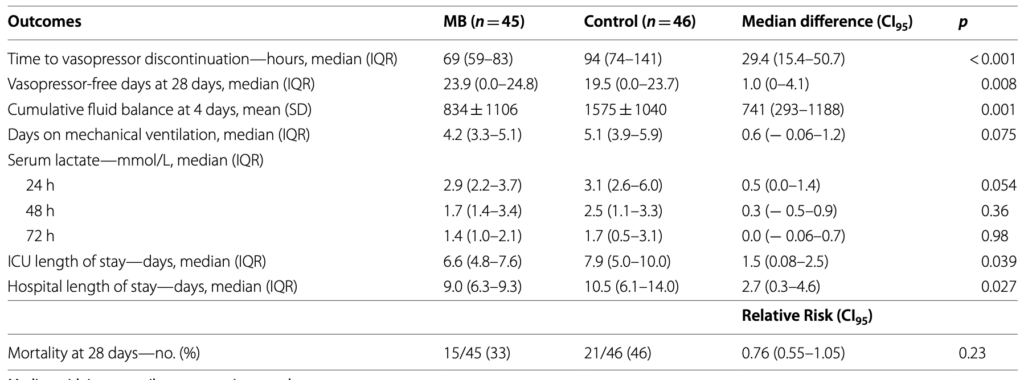
- Time to vasopressor discontinuation was shorter in the methylene blue group
- Noradrenaline dose decreased in the methylene blue group in the first 4 days
- Less patients in the methylene blue group required required re-initiation of noradrenaline within 48 hours of discontinuation.
Secondary outcomes
The methylene blue group had:
- More vasopressor-free days
- Lower cumulative fluid balance
- Shorter ICU and hospital stay
There were no adverse effects with using methylene blue. Conclusions could not be made on mortality as it was underpowered to do this.
Conclusions
This was a single centre study, but it was randomised and placebo controlled.
- The fluid loading doses was given in ml/kg. It was similar in both groups, but we don’t know how much fluid in total patients received.
- The noradrenaline doses were quite high ie., 0.45 mcg/kg/min in the methylene blue group vs 0.37 mag/kg/min in the placebo group ( although this favours a better outcome with methylene blue)
- in a 70 kg patient this would be 31mcg/min in methylene blue group and 25.9 mag/min in the placebo group.
- Vasopressin use was similar in the two groups.
- The dose of methylene blue was purposely lower than in other studies, to avoid cumulative doses that occur with continuous infusions and the associated negative effects on cardiac, pulmonary, kidney and liver function.
I read this study with interest, primarily as I have had shocked patients that have had large requirements for vasopressors and have had the associated adverse effects of peripheral ischaemia and arrhythmias. Although this was primarily an ICU study and more work needs to be done, it is something that we can use in the emergency department, given the amount of time sepsis patients stay in the department. Perhaps the earlier use, could result in less time in ICU (69 hours vs 94 hours in this study. I will follow more studies with interest.
This blog was first published on resus.com.au by Dr Peter Kas
\References
- Ibarra-Estrada M et al. Early adjunctive methylene blue in patients with septic shock: a randomised controlled trial. Critical Care 2023 27;110: 1-10. PMID: 36915146
- Kirov MY et al. Infusion of methylene blue in human septic shock: a pilot, randomized, controlled study. Crit Care Med. 2001;29:1860–7. PMID: 11588440
- Memis D al. The influence of methylene blue infusion on cytokine levels during severe sepsis. Anaesth Intensive Care. 2002;30:755–62. PMID: 12500513
- López A et al. Multiple-center, randomized, placebo-controlled, double-blind study of the nitric oxide synthase inhibitor 546C88: effect on survival in patients with septic shock. Crit Care Med. 2004;32:21–30. PMID: 14707556