Status Epilepticus in a Child
Mar 27, 2024The CASE
A 7 yo child is brought in by ambulance after having tonic clonic seizures that morning. The whole family had been travelling for a holiday. Her mother tried to wake her in the morning, but she was not responding much, so left her sleep a little longer. Approximately one hour later she was found to be having a tonic clonic seizure. The Ambulance were called.
The child has no past medical history although her siblings have had recent viral symptoms. Paramedics have treated with 5 mg midazolam IM and the tonic-clonic component of the seizure appears to have settled.
On arrival to the Emergency Department, the patient is afebrile, tachycardic at a rate of 126 bpm with a BP of 105/55 and a respiratory rate of 26/min and Saturations are 100% on 10L oxygen. Examination reveals pinpoint pupils with divergent gaze, and a GCS of 5/15. Heart sounds are dual, chest is clear and abdomen is soft, with no rash seen. Although the tonic clonic component of the seizure is settled, there is occasional shaking of the arms and the patient has not improved in conscious state. Pupils are still divergent…. The seizure continues. Blood glucose is normal.
What do we do next? The patient is still seizing.
Should we intubate at this point?
Should we give antivirals/antibiotics?
What is the most likely cause in an otherwise well child?
In this case:
Further midazolam was given
IV Levatiracetam was added
Ceftriaxone and Acyclovir were given
Phenytoin was then given
The seizure continued, so the team proceeded to Rapid Sequence Intubation with Propofol and Rocuronium
An infusion of Midazolam was commenced
Dexamethazone was given.
The child was transferred to a paediatric facility.
Let’s have a look at an approach.
Having a standardised approach is key. Not having such an approach is associated with increased morbidity and mortality (1).
Definition of Status Epilepticus
The definition varies depending on the type of seizure, however for a tonic-clonic seizure, there are two time points to know about(2):
Time Point 1: This is the time at which we consider the seizure to be prolonged. It is the point where we need to intervene, to avoid going to the next time point. This is 5 minutes.
Time Point 2: This is the time after which neurological injury occurs. This is 30 minutes
How do we approach this patient?
This is not a textbook. This is real life, along with the stress and the chaos that sometimes accompanies it. The Pathophysiology, although important, is not important in the clinical setting. What’s important here is getting on and doing the things that will minimise damage. In this case, the seizure may have been going on for at least an hour.
The basic approach involves:
- Stopping the seizure and at the same time,
- Treating the underlying cause, understanding that by doing this, the seizure may stop anyway.
Aetiology
In about 15% of patients, we may never know the cause.
In the acute presentation, with no previous pathology, the most common causes include:
- Hypoglycaemia
- Infection: Beware meningitis, as only a small proportion of children present with fever.
- Trauma
- Tumour
- Underlying epilepsy with inadequate treatment
- Hypoxia
- Electrolyte imbalance
- Toxicological: this can include a large number of potential toxicological ingestions including
In this case, infection is highest on the list.With these potential causes in mind, but no single one being obvious we progress quickly through what we can do. I think it’s good to develop an approach that is rapid and takes care of the most important aspects of the condition. It treats the most important potential causes. We then have time to come back to other causes.
An Approach
 Anything Reversible?
Anything Reversible?
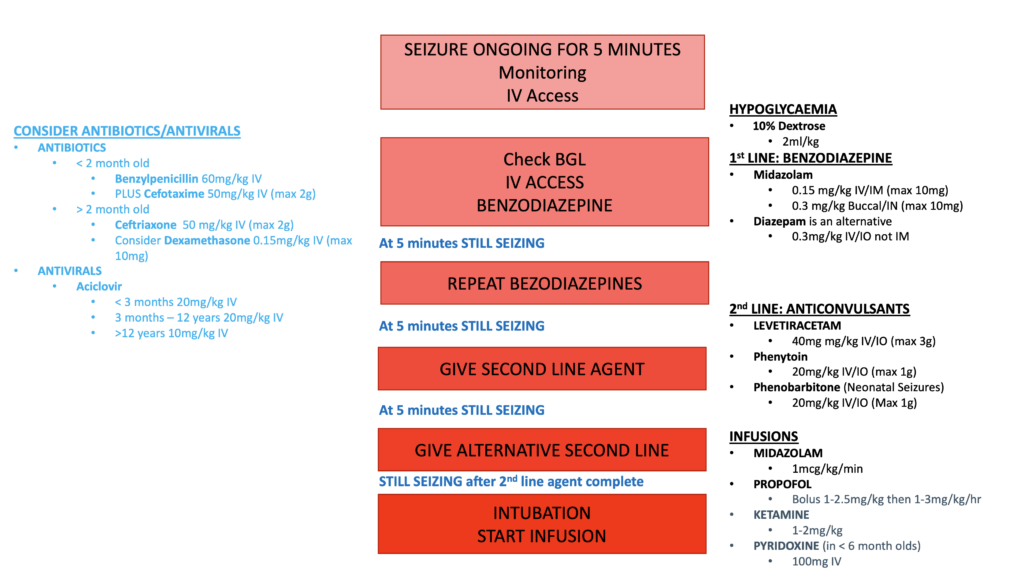
Blood Glucose Level is the most important: Is this hypoglycaemia? If <2.6mmol/L treat. I will often treat any patient with BSL < 3mmol/L. 2ml/kg of 10% Dextrose.
Anti-convulsants
- Midazolam 0.2mg/kg IM/IV/buccal/intranasal, is a popular choice as it can be given via all routes.
- Levetiracetam 40mg/kg IV (4500 mg max)
- I will consider a second anticonvulsant if this is not working ie Phenytoin IV 20 mg/kg, (max 1500 mg/dose)
Antibiotics/Antivirals
Give these at the same time as the anticonvulsants if concerned about meningitis. (Refer figure).
Infusions for Deeper Sedation
At this point, we need to move to an infusion, to stop the seizure. The patient will have a decreased conscious state from the benzodiazepines given previously. These infusions will further sedate, so intubation is needed.
In some cases the use of propofol for induction may resolve the seizure, however we don’t tend to use a large dose, that might do that. Beware, as the patient has already had a significant amount of benzodiazepines and a large dose of propofol may drop the blood pressure.
Infusions can be of Propofol, Midazolam or Ketamine. Consider Pytidixine in < 6 yo (refer figure). Read more about Ketamine in Refractory Seizures.
At this point we have done all that we can in the emergency department.
This is a stressful time for all staff, control the noise and let all your team know what’s happening and assign a team member to the family, so they know what’s happening. A debrief at the end of the day may be helpful.
References:
- Chin RF, et al. Inappropriate emergency management of status epilepticus in children contributes to need for intensive care. J Neurol Neurosurg Psychiatry. 2004 Nov. 75(11):1584-8.
- Trinka E, et al. A definition and classification of status epilepticus–Report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. 2015 Oct. 56 (10):1515-23.
- The Royal Children’s Hospital Melbourne Clinical Guideline.
Join Our Free email updates
Get breaking news articles right in your inbox. Never miss a new article.
We hate SPAM. We will never sell your information, for any reason.